2024 general elections : What are the plans of the candidates on the end of life and old age?
Apart from the presidential majority party who would like to debate the bill on the end of life as a priority issue, the subject is not at the heart of the intentions of the different political parties for the general elections to be held on 30th June and 7th July 2024. As for old age, the issue has been swept under the carpet for these elections.
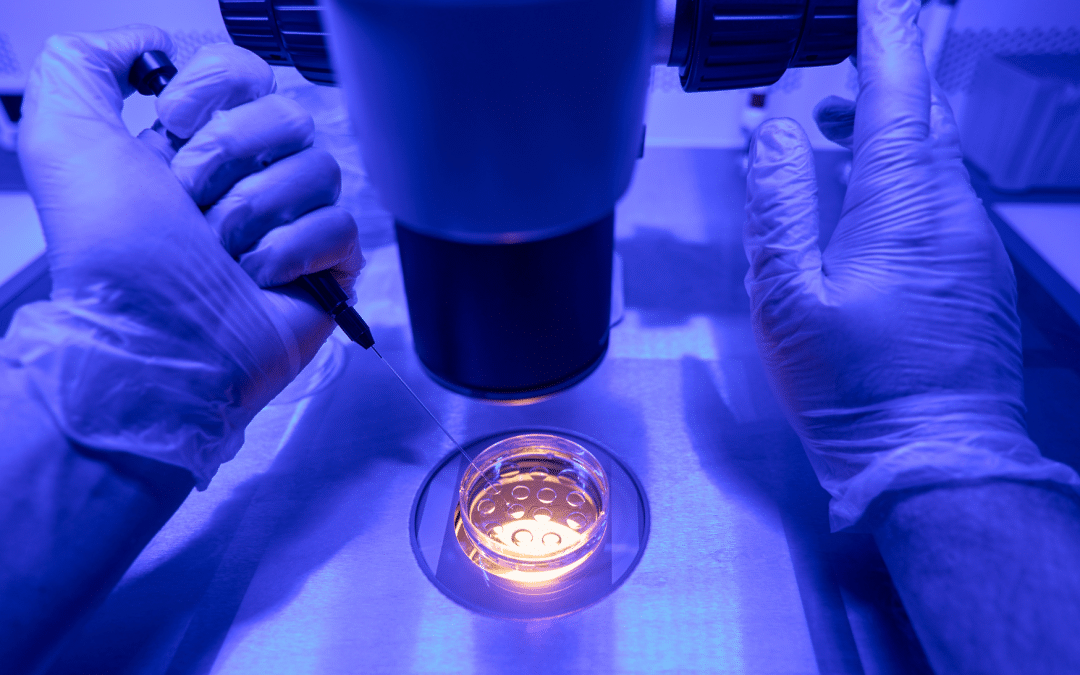
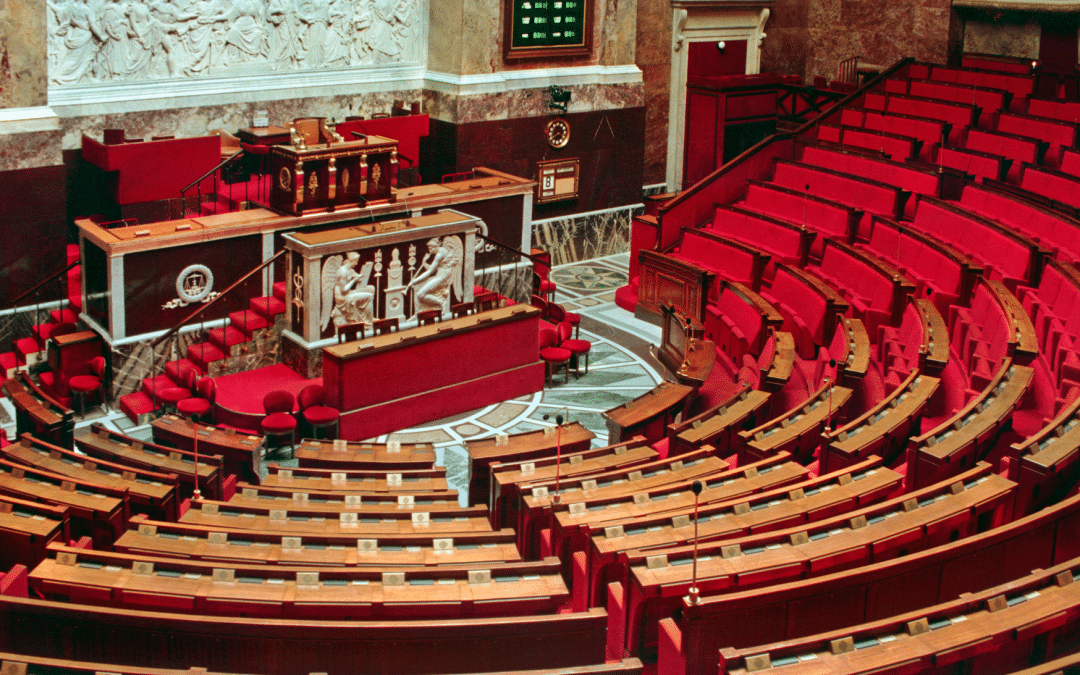
The dissolution declared by the French President on 9th June put a halt on the end of life bill, for which the public session debates at the National Assembly had started on 27th May. The parliamentary candidates are divided on the importance to be afforded to the issue in their programmes.
A priority for the presidential majority
In the event of victory by the presidential party whose title is now “Ensemble pour la République” (Together for the Republic), Gabriel Attal announced that the text on the end of life, authorising “assistance in dying” would be put back on the agenda of the new Assembly as early as July, before the Olympic Games. When interviewed by France Inter on Monday 24th June, the ex-president of the National Assembly Yaël Braun-Pivet stated that she would again register the text on the end of life as a priority issue, as the text is “impatiently awaited by the people”.
Total absence in the other programmes
Nevertheless, that position is isolated in the debates surrounding the elections. The end of life does not appear in the programme for the “Nouveau Front Populaire”, even though several voices have been heard within the left-wing alliance in favour of a bill for euthanasia or assisted suicide. Fabien Roussel, the national secretary for the Parti Communiste Français (French Communists), has called for resuming the parliamentary debates. The LFI MP Hadrien Clouet, who is standing for re-election, has taken a commitment to resubmit the bill if he is re-elected.
The programmes for Les Républicains (LR) and the Rassemblement National (RN) are silent on the question. Within those parties, the candidates themselves are divided. Certain of them have expressed their will to develop palliative care. What is clear, is that the end of life is not a key issue for this election campaign.
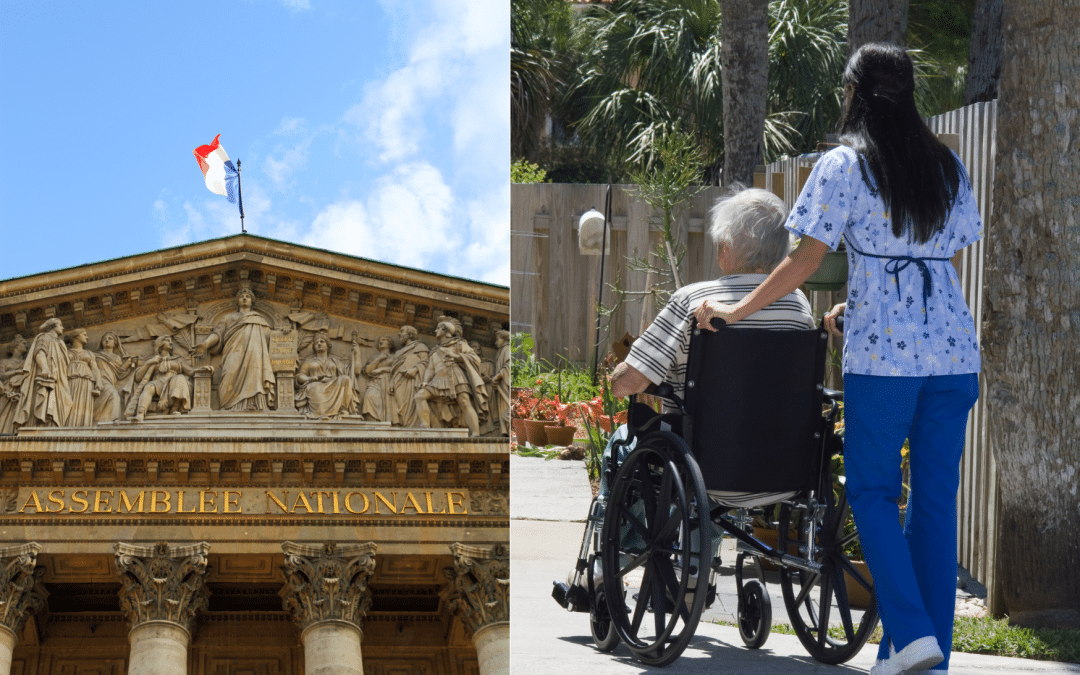
Old age, the forgotten issue for these elections
In view of the enormous challenge presented by the ageing of the French population and the crisis already being experienced by the old age sector, one might have expected that the issue would be addressed by the different political groups. A law on old age had been announced back in 2018 by Emmanuel Macron and again promised in November 2023 by the then Prime Minister Elisabeth Borne. However, apparently old age is not a popular subject.
On the subject, there are a mere two lines in the programme for the “Nouveau Front Populaire”, who propose to “launch an old age plan by renovating the EHPADs (old people’s homes), by increasing the numbers and training professionals for old age”. The 12-page programme for “Ensemble pour la République” makes no mention of the subject. The “Rassemblement National” (RN) under the heading of health proposes “to reinforce the support for relative-carers” but without saying how.
The election candidates would be well advised to consider the 2024 Ifop/Synerpa survey on old-age and the challenges represented by ageing, published on Monday 24th June. According to that survey, nearly 7 out of 10 French nationals consider that the public authorities have not done enough to improve the situation in EHPADs (69 %). They could also look at the results of the RH & Finances survey published on 14th June by the FNADEPA (National federation of the associations of directors of establishments and services for the elderly).
This identifies a new deterioration of the financial situation of establishments and services for the elderly, irrespective of their public or private status. According to the survey conducted on 1,500 FNADEPA members, 65 % of the ESMS were in deficit in 2023 and 58 % were short of personnel.
In this context, Alliance VITA recalls that, among the 5 priority issues for these elections, the most critical is the urgency to pass a law on solidarity for the elderly and the need to guarantee access to palliative care for all. These questions will not be avoidable by the next government.